Correlation between O6-methylguanin-DNA methyltransferase (MGMT) and p53 in clinical response
INTRODUCTION
Pancreatic ductal cancer (PDA) was the fourth leading cause of death from cancer in the United States in 2010 with a poor prognosis: the 5-year survival rate is 6% in Europe and the United States. FOLFIRINOX an association of fluorouracil, leucovorin, irinotecan and oxaliplatin has become a standard therapeutic in metastatic pancreatic adenocarcinoma for selected patients with good performance status below 70 years old by increasing median overall survival at 11,1 months (1).
Currently, the studies seek to enhance therapeutic efficacity by studying molecular targets. Unfortunately, there is little information regarding biomarkers for FOLFIRINOX regimen at the current time (2).
Mutations in genes encoding proteins involved in DNA damage repair promote to genetic instability and cancer. And the identification of impaired DNA repair in different cancers has allowed the development of treatments that use DNA repair defects in certain patient populations with for example, the PolyADP-ribose polymerase (PARP) inhibitors, that inhibit the activity of PARP proteins which are involved in a variety of DNA damage repair pathways. Clinical studies have shown that BRCA 1/2-deficient tumours are sensitive to PARP inhibitors and platinium agents by synthetic lethality (3).
One of the most supported mechanisms of tumor resistance to DNA-damaging agents is the overexpression of the repair protein MGMT. MGMT protects cells against mutagenic and cytotoxic alkylation DNA damage and represents a significant barrier to the successful treatment of patients with cancer (4-5).
MGMT levels have been reported previously to be elevated in advanced adenocarcinoma of the pancreas contrasted to normal pancreatic tissue (6). The MGMT gene, located on chromosome 10, encodes a repair enzyme excising the alkyl groups of the o6 position of guanine.
During the process, the alkyl group is transferred to the enzyme, which becomes irreversibly inactive and comes to be degraded. This protein rapidly reverses formation of adducts at the o6 position of guanine and averts the formation of lethal DNA cross-links induced by alkylating agents.
Recently, it has been reported that cytotoxic activity of temozolomide, an alkylating agent, is correlated with a loss of MGMT expression measured by immunohistochemistry both in pancreatic endocrine tumors and glioblastoma (7-8).
The loss of MGMT expression results from the hypermethylation of the MGMT promoter cysteine-phosphate-guanine (CpG) island (4). The efficacy of camptothecins is explained only in part by their ability to damage DNA.
It has been shown that MGMT may act to modulate cytotoxicity of camptothecin-derived topoisomerase I inhibitors (CPTs) (9).
Interestingly; loss of MGMT expression could render cells more sensitive to CPTs through the modulation of protein-linked DNA breaks (9).
Platinums are cytotoxic by virtue of the formation of DNA cross-links preferentially at the N7 position of guanine and adenine. Their activity is not affected by the presence of the DNA-repair protein o6-alkylguanine DNA alkyltransferase (10).
However, it has been suggested that platinum compounds caused substantial and prolonged MGMT depletion and play a role in the down regulation of MGMT expression and this may increase the sensitivity to CPTs (11-12).
Furthermore, Murakami et al (13) have observed an enhancement of the anti-tumor effect of 5-Fluorouracil in response to MGMT depletion in colon and oral cancer cells lines. So, a key role of the MGMT as a mechanism of resistance to chemotherapy could be involved in pancreatic adenocarcinoma.
P53 is one of the most important tumor suppressor proteins identified (14). It is mutated in most of human tumors and represents an important step in pancreatic tumor progression. The lack of expression of p53 is possibly associated with a post-MGMT mechanism of tumor resistance because p53 is involved in regulation of cell cycle checkpoint in response to DNA damage (15). It has been reported that decreased MGMT expression is correlated with p53 activation, and this could reduce pancreatic tumor growth. Nonetheless, the specific roles of MGMT and p53 in the therapeutic response of human pancreatic cancer are unknown. At our knowledge, MGMT and p53 expression has never been studied in patients treated by FOLFIRINOX combination. In a preliminary study, we want investigate the prevalence of MGMT status in metastatic adenocarcinoma pancreatic and search if a any relationship exists between the tumor expression of MGMT and p53 and therapeutic response and survival in patients treated with FOLFIRINOX regimen.
PATIENTS AND METHOD
Patients were eligible to be included in the study if they were 18 years old of age or older and had histologically confirmed, measurable metastatic pancreatic adenocarcinoma treated by first-line treatment FOLFIRINOX in the University hospital of Angers (France). Other inclusion criteria were a life expectancy of at least 3 months and an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 or 1. The data were retrospectively collected.
Clinical Data At the inclusion of patients, number parameters were collected: the age at diagnosis, the sex of patients, the location of the cancer in pancreas and metastatic sites, the date of beginning and end date of FOLFIRINOX, the number of cycles of chemotherapy, the received dose of chemotherapy, the computed tomodensitometric scans (CT scans) evaluations at 6 (C6) and 12 cycles (C12), the date of progression disease, the date of death. An inform consent was collected in alive patients.
RESULTS
Clinical data
Between September 2011 and June 2015, 30 patients with metastatic pancreatic adenocarcinoma were recruited in the study The average age of patients was 65.3 years (range 45.6 to76). The location of the pancreatic tumors was mainly the head of the pancreas (80.0%) and the most frequent metastatic site was the liver (76.6%). The median number of treatment cycles administered was 12 (range 3 to 16). The median relative dose intensity of fluorouracil, irinotecan and oxaliplatin were 85%, 80% and 76% respectively. 9 patients were treated in second line (Table I).
MGMT and status
Tissue collections were collected from 9 EUS-FNA pancreatic, 14 liver biopsy and 7 pancreaticoduodenectomy. 76.7% tumors were MGMT positive (figure 2). Concerning to the expression of p53: 23.3% tumors had negative expression, 26.7% had a weak expression, 13.3% had moderate expression and 36.7% had a diffuse expression.
After 6 cycles:
Among patients who have tumors MGMT positive: 30.4% have a complete or partial response, 52.2% have a stable disease and 17.4% have a progressive disease.
Among patients who have tumors MGMT negative: 14.3% have a complete or partial response, 71.4% have a stable disease and 14.3% have a progressive disease. There was no significant difference in response rate at 6 cycles (p=0.836).
Among patients who have tumors that expressed negative or weak p53: 20.0% have a complete or partial response, 60.0% have a stable disease and 20.0% have a progressive disease.
Among patients who have tumors that expressed moderate or strong p53: 33.3% have a complete or partial response, 53.3% have a stable disease and 13.3% have a progressive disease. There was no significant difference in response rate at 6 cycles (p=0.78).
After 12 cycles
Among patients who have tumors MGMT positive: 23.8% have a complete or partial response, 33.3% have a stable disease and 19.1% have a progressive disease.
Among patients who have tumors MGMT negative: 14.3% have a complete or partial response, 71.4% have a stable disease and 0.0% has a progressive disease. There was no significant difference in response rate at 12 cycles (p=0.435) depending on the positive or negative expression of MGMT.
Among patients who have tumors that expressed negative or weak p53: 20.0% have a complete or partial response, 40.0% have a stable disease and 13.3% have a progressive disease.
Among patients who have tumors that expressed moderate or strong p53: 23.1% have a complete or partial response, 46.2% have a stable disease and 15.4% have a progressive disease. There was no significant difference in response rate at 12 cycles (p=0,949).
PFS and OS
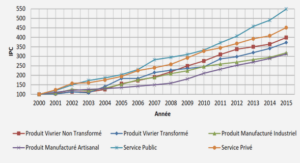
The progression-free survival and the overall survival were not significantly different on depending MGMT status (Figure 4).
At the end of the study, 60.8% patients with tumors MGMT positive died and 42.9% with tumors MGMT negative. The average OS in patients with tumors MGMT positive was 522.3 +/- 68.9 days and in patients with tumors MGMT negative 618.0 +/-146.4 days. There was no significant difference in OS depending on the positive or negative expression of MGMT (p=0.39).
The average PFS in patients with tumors MGMT positive was 257.0 +/- 38.2 days and in patients with tumors MGMT negative 325.7 days +/-19.1 days. There was no significant difference in PFS depending on the positive or negative expression of MGMT (p=0.112).
DISCUSSION AND CONCLUSION
PDA is one of the major causes of cancer death worldwide and the treatment of metastatic disease remains challenging as only certain patients benefit from advances made with the intensified chemotherapy regimen FOLFIRINOX (1). Up to date, no established approach for prediction of treatment response exists (2,15).
Recently, the methylation status of the MGMT gene promoter was an important biomarker highlighted in pancreatic endocrine tumors (7) increasing progression-free survival and overall survival in alkylant use (17-18). Moreover the blockade of MGMT expression could lead to reduce pancreatic tumor growth in mice model (19).
Correlations between promoter methylation and response to chemotherapy with alkylating agents are explained by the assumption that DNA methylation of a cysteine-phosphate-guanine (CpG) island within the MGMT promoter directly leads to a repression of MGMT transcriptional activity and MGMT protein expression (6). In addition, platinium salts may modulate the activity of MGMT (12).
However, MGMT methylation does not confer sensitivity to the killing action of alkylating agents if the tumor is also MMR deficient (20). It has been previously reported association between MMR genes variants and overall survival (21) supporting a role for DNA MMR deficiency in pancreatic cancer progression and defective MMR has been reported in up to 13% of sporadic pancreatic cancer (10).
Genetic variations in MGMT were correlated with overall survival in patients with localized disease (21). So, it was interesting to check the frequency of MGMT deficiency in pancreatic adenocarcinoma and to study a possible correlation with therapeutic efficacy. MGMT deficiency is rare in metastatic pancreatic adenocarcinoma (23.3% in our study) (6). MGMT status assessed by immunohistochemistry failed to modulate response rate, progression free survival and overall survival in patients treated by FOLFIRINOX. Notably, MGMT deficiency was not correlated with a poor prognosis in contrast with previous observation in other tumors (22).
This could be explained by a better activity of irinotecan in MGMT negative patients. Another hypothesis to explain the effectiveness of FOLFIRINOX in pancreatic adenocarcinoma is that oxaliplatin as cisplatin could perform a downregulation on MGMT expression (23) and sensitize tumor cells to CPTs. MGMT antibodies does not necessarily indicates a MGMT deficient phenotype because the presence of connective tissue and normal-appearing pancreatic components have markedly lesser MGMT (6).
The true methylation status of MGMT by molecular techniques should however be investigated before definitive conclusions of this subject. An analysis of MMR genes would be interesting.
|
Table des matières
INTRODUCTION
PATIENTS AND METHOD
ERROR! BOOKMARK NOT DEFINED.
RESULTS
1. Clinical data
2. MGMT and p53 status
3. Objective response
3.1. After 6 cycles
3.2. After 12 cycles
3.3. PFS and OS
4. Relationship between MGMT and p53
DISCUSSION AND CONCLUSION
![]() Télécharger le rapport complet
Télécharger le rapport complet